Advanced Shock Wave
Lithotripsy
One of the most effective, non-invasive methods for kidney stone treatment.
About the Doctor
Dr. Ahmad Ahmadov has been practicing as a certified urologist and extracorporeal shock wave lithotripsy specialist in leading clinics since 2006.
He combines advanced medical technologies and modern approaches in ESWL with personalized treatment strategies, providing patients with a high level of safe and effective medical care.
His professional experience, precision-based approach, and patient-oriented treatment philosophy distinguish him as one of the most trusted specialists in the field.

Dr. Ahmad Ahmadov
Certified Urologist & ESWL Specialist
20+ Years of Experience
25,000+ Successful Procedures
About Kidney Stone Disease
Kidney stone disease (urolithiasis) is one of the current problems in urology. The problem of the disease's widespread occurrence and recurrence of stone formation is relevant. According to statistics, approximately 5–15% of the world's population has urolithiasis to some degree. Crystalluria (the condition where stone-forming substances exceed normal levels and begin to deposit) is common. The patient may be asymptomatic and may feel well for a long time without any symptoms, feeling fine. Sometimes a patient may visit a doctor with kidney pain and upon examination be told they have a stone that has been present for a long time.
Modern treatment of kidney stone disease offers many treatment methods. Advanced methods in developed countries involve wide use of minimally invasive techniques, applied only in specific cases. Currently, the most commonly used minimal invasive methods are available. Among these methods, Extracorporeal Shock Wave Lithotripsy (ESWL) is particularly widely used and is one of the effective methods. This method does not require any incision or surgical intervention; shock waves are directed from outside the body and afterward the fragments are naturally excreted through urine. The procedure is non-invasive, safe, and can be performed on the same day, allowing the patient to go home. For small and medium-sized stones, this is the most preferred method. When extracorporeal lithotripsy is not possible, endoscopic methods such as URS (ureteroscopy) and percutaneous nephrolithotomy (PNL) are used. Stone formation mechanisms can be explained as follows: initially, the basic organic core material forms, then layers of stone-forming mineral substances build up on it. Stones are classified according to their composition as follows:
- Urate stones (uric acid salts)
- Oxalate stones (oxalate acid salts)
- Mixed stones (urate-oxalate)
- Phosphate stones (phosphate acid salts)
- Cystine stones (cystine amino acid metabolites)
Urate, oxalate, and mixed stones are the most commonly encountered types (90%).
ESWL necə işləyir
Extracorporeal Shock Wave Lithotripsy uses focused shock waves to break kidney stones into small fragments.



Shock Wave Generation
The lithotripter generates precisely focused shock waves.
Stone Fragmentation
Focused waves break the stone into tiny fragments.
Fragment Migration
Small fragments travel through the ureter to the bladder.
Natural Excretion
Fragments are naturally excreted through urination.
ESWL process under ultrasound control
Before
After
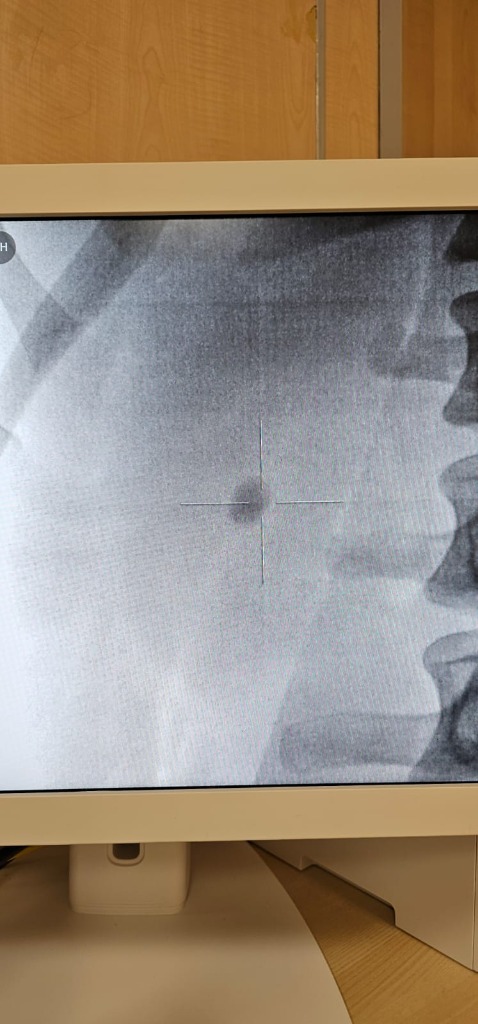
Before
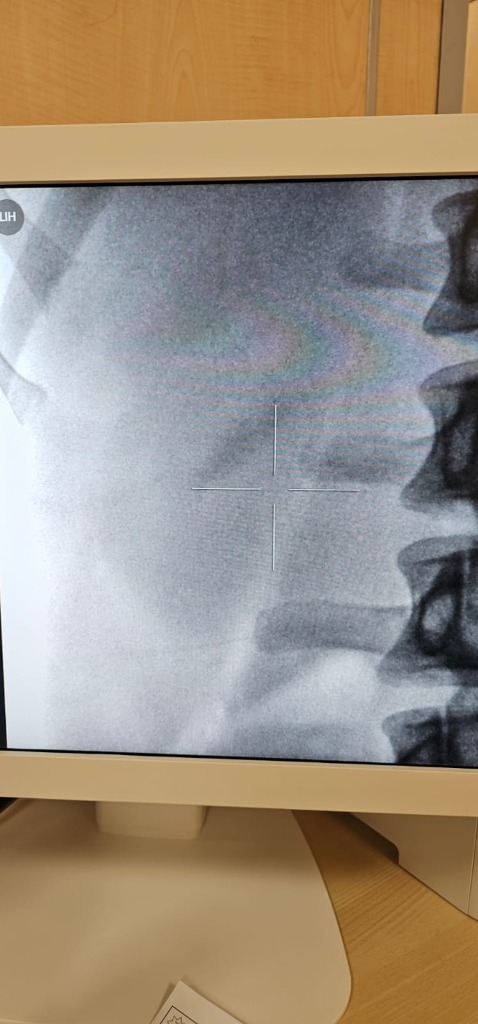
After
Treatment Methods
1. Prophylactic and Conservative (Lifestyle and Medication) Treatment:
- *Diet and lifestyle changes.
- Daily fluid intake increase (it is recommended to drink 2–2.5 liters of water per day, appropriate for diuresis) to reduce crystallization and stone formation risk.
- Increasing sodium intake via kidneys reduces calcium in urine, and calcium plays a key role in stone prevention.
- Increasing protein intake in the diet lowers uric acid and calcium levels, reducing oxidite stone formation risk.
- Reducing oxalate-rich foods (spinach, beets, rhubarb, chocolate) helps decrease adequate calcium retention and reduces oxalate stone formation risk.
- Metabolic evaluation is the basis for selecting specific diet and lifestyle correction; repeat stone formation prevention is essential.
- *Medical treatment: (Be careful with self-medication!!!)
- Urinary alkalinization and pH balancing — citrate preparations (potassium citrate) reduce the risk of uric acid stone formation.
- Diuretic preparations — thiazide diuretics lower calcium levels in urine and are used for stone prevention.
- Urate stone treatment — allopurinol reduces uric acid levels, lowering urate stone formation risk.
- Anti-infection antibiotics — used for struvite stone treatment and prevention.
- Individual treatment plan — each patient's metabolic profile is considered for personalized stone prevention.
2. Extracorporeal Lithotripsy (Non-Invasive Method):
A modern, minimally invasive method using shock waves to break kidney and ureteral stones into fragments without any surgical intervention. The procedure is performed using a special device, and the stone fragments are naturally excreted through urine.
Advantages of the procedure:
- Painless and safe — performed under local anesthesia and is a mild, simple procedure.
- Short duration and quick recovery — outpatient procedure, patient can go home the same day.
- High effectiveness — effective for small and medium-sized stones (80–90% success rate).
- Minimal complication risk — avoids surgical intervention, keeping complication rates very low.
- Individual approach — treatment is tailored to each patient's stone size and location.
Extracorporeal lithotripsy provides a painless, safe, and quick solution for stone removal. If you are looking for comfort and fast recovery, this is the ideal method.
3. URS — Ureteroscopy (Endoscopic Method):
URS (ureterorenoscopy) is a minimally invasive endoscopic procedure for direct visualization and removal of stone fragments from the ureter. A thin endoscope is inserted through the urethra into the ureter to locate and remove or fragment stones using laser energy.
Recommended for:
- Ureteral stones that cannot be treated with ESWL.
- Stones in the lower and middle ureter.
- When ESWL has been unsuccessful after multiple sessions.
- Stones requiring direct visualization for removal.
4. Percutaneous Nephrolithotomy (Minimally Invasive Surgical Method):
This method is used for removing large (staghorn) and very dense stones from the kidneys using a minimally invasive surgical approach. The choice is made according to the patient's individual situation.
Recommended for:
- Large, staghorn, and very dense stones.
- When extracorporeal lithotripsy is not technically possible, for example:
- very large stone volume,
- horseshoe kidney,
- other anatomical and medical reasons.
Advantages of ESWL
Why ESWL is the preferred choice for kidney stone treatment.
Non-Invasive
No incisions, no needles, no instruments entering the body.
Virtually Painless
Most patients experience only mild discomfort.
Quick Procedure
Treatment typically takes 30-60 minutes.
High Success Rate
Success rates of 70-95%.
Minimal Recovery
Return to normal activities within 1-2 days.
Proven Technology
Used worldwide for over 40 years.
Pediatric Lithotripsy
We are the only center in the Republic performing lithotripsy in children from infancy.
Sedation for Young Children
In children under 8–9 years of age, the procedure is performed under sedation in the presence of a qualified anesthesiologist.
Superior Outcomes in Children
Due to the shorter and more elastic ureter, treatment outcomes are often even better than in adults.
Pediatric Contraindications
Specific pediatric contraindications include congenital anomalies of the ureters.
Medical Information
Comprehensive medical details about ESWL treatment.
⚠Important Information About Extracorporeal Lithotripsy
Extracorporeal lithotripsy — is a method of breaking kidney and ureteral stones into fragments using minimal invasive approach. However, the patient should be aware of the following:
• The method does not guarantee 100% stone clearance with minimal pain. After the session, some stone fragments may pass naturally through the urinary tract in a different pattern. The process may vary: some fragments pass easily, while ISA can cause severe pain, renal colic, nausea, and may require medical attention.
• If pain becomes unbearable, the doctor may recommend inserting a ureteral stent (Double-J stent) before or after ESWL to allow easier fragment passage and reduce the risk of obstruction.
• In some cases URS (ureteroscopy) may be necessary. If stone fragments cause blockage or the ureter becomes obstructed, URS may be required. URS is used to remove remaining fragments from the ureter.
After the procedure, it is recommended to drink plenty of fluids (2–2.5 liters) and follow the medical regimen prescribed by your doctor.
- the stone's composition (density) — dense stones, such as cystine or calcium oxalate monohydrate, fragment into larger pieces and take longer to pass,
- the stone's location — stones in the lower kidney or distal ureter can take longer and cause more discomfort,
- anatomical features of the urinary tract.
• Predicting exact outcomes is not possible — stent, URS, or repeated lithotripsy sessions may become necessary. Outcomes can only be determined after post-treatment observation.
Vacibdir: distansion litotripsiya — effektiv, təhlükəsiz və müasir metod olsa da, prosedurun fərdi xüsusiyyətlərini başa düşmək və müalicə planına hazır olmaq vacibdir.
Kidney Stones 4-20mm
Stones in the renal pelvis or calyces within this size range respond well to ESWL.
Upper Ureteral Stones
Stones in the upper third of the ureter can be effectively treated.
Stones Under 2cm
Most stones under 2cm are ideal candidates.
Non-Obstructing Stones
Stones not causing complete obstruction.
Stone Density Below 1300–1400 HU
Stones with CT density under 1300–1400 Hounsfield Units are more fragile and respond well to ESWL. Higher-density stones may resist fragmentation.
Pregnancy
ESWL is not performed on pregnant patients.
Bleeding Disorders & Anticoagulants
Patients with bleeding disorders or on anticoagulant therapy. Anticoagulants must be discontinued at least 5 days prior.
Active UTI
Active urinary tract infection must be treated first.
Aortic Aneurysm
Patients with aortic aneurysm near treatment area.
Cardiac Pacemaker
Shock waves can interfere with pacemaker function. Cardiologist clearance is required before ESWL.
Hematuria
Blood in urine, typically resolves in 24-48 hours.
Stone Fragments
Larger fragments may require additional sessions.
Steinstrasse
Accumulation of fragments in the ureter. May require stenting or URS.
Mild Discomfort
Temporary flank pain or bruising.
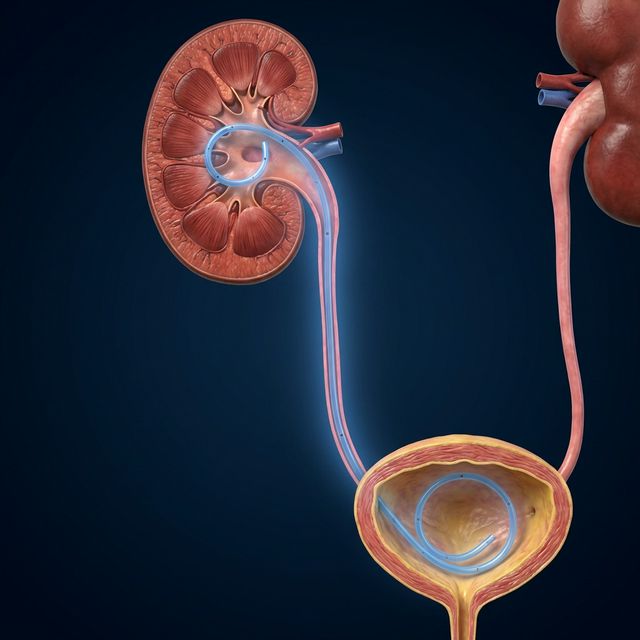
What is a Stent?
A thin, flexible tube placed inside the ureter to maintain urine flow.
When is it Needed?
- Large stones (>15mm)
- Ureteral narrowing
- Solitary kidney
- Infection with obstruction
- After complicated lithotripsy
Why is it Placed?
Ensures continuous drainage. Removed after 1-4 weeks.
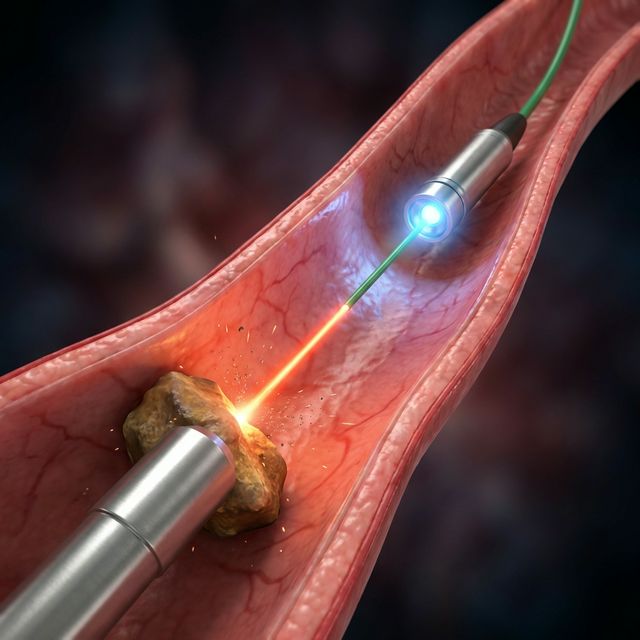
What is URS?
URS (ureterorenoscopy) is a minimally invasive endoscopic procedure for direct visualization and removal of stone fragments from the ureter.
Stent Placement
URS Procedure
Technical Limitations
Due to individual anatomical features, excess body weight, or specific stone location, ESWL may be technically impossible in certain patients. In such cases, the physician will provide professional recommendations and refer the patient to the appropriate specialist.
Our Equipment
We use the Storz Modulith SLX-F2 — one of the world's most advanced electromagnetic lithotripters.


Storz SLX F2 — современный высокоэффективный литотриптор для дистанционного дробления камней почек и мочеточника. Аппарат оснащён инлайн-УЗИ наведением, позволяющим в реальном времени точно визуализировать конкремент и контролировать процедуру. Дополнительная рентген-навигация обеспечивает двойной контроль позиционирования. Система с изменяемым фокусом ударной волны позволяет адаптировать воздействие под размер и глубину камня, повышая эффективность и безопасность лечения.
Book Your Appointment
Schedule Consultation
Post-Lithotripsy Recommendations
Following these guidelines will help optimize stone fragment passage and recovery.
Adequate Fluid Intake
Consume up to 2–3 liters of fluids per day.
Maintain Physical Activity
Stay moderately active. Avoid prolonged lying or sitting.
Monitor Bowel Function
Prevent constipation and flatulence.
Warm Baths for Lower Ureteral Pain
Warm hip-level baths may help relieve ureteral spasm.
Pain Management
During fragment passage, pain may vary. Pain must be managed with prescribed analgesics.
Repeat Sessions
The need for repeat sessions is determined at follow-up examination after 10–15 days.
Frequently Asked Questions
Everything you need to know about ESWL treatment.
Myths vs. Facts
Let's debunk common misconceptions about lithotripsy.
ESWL is extremely painful and requires full surgery
Click to see the truth →ESWL is non-invasive and virtually painless.
Click to see the myth →Kidney stones always come back after ESWL
Click to see the truth →ESWL effectively destroys stones. Recurrence depends on lifestyle.
Click to see the myth →Shock waves damage the kidneys permanently
Click to see the truth →Modern lithotripters use precisely focused, low-energy waves.
Click to see the myth →You need weeks of bed rest after ESWL
Click to see the truth →Most patients return to normal activities within 1-2 days.
Click to see the myth →Drinking beer helps dissolve stones
Click to see the truth →Alcohol doesn't dissolve stones and can dehydrate you.
Click to see the myth →ESWL is only for kidney stones
Click to see the truth →Modern ESWL is effective for ureteral stones too.
Click to see the myth →Procedure Videos
Watch real lithotripsy sessions performed at our center.